
By CCHR International
March 2026
Data obtained by CCHR International through Freedom of Information Act (FOIA) requests from 32 states found that 2,999,084 children aged 0–17 were prescribed psychiatric drugs under Medicaid—the federal health program for low-income families—in 2023, including 270,196 children aged 0–5, costing taxpayers $1.78 billion.
By comparison, the IQVIA Total Patient Tracker—one of the most comprehensive and widely used sources of U.S. prescribing data—reported 6,155,852 children (0–17) nationwide prescribed psychiatric drugs in 2020, meaning nearly half that total is already accounted for by Medicaid children in just 32 states, with 18 states still unreported.
This indicates that Medicaid—the program serving low-income children—is the primary driver of psychiatric drug prescribing among U.S. youth, with nearly 3 million children identified in just 32 states alone.
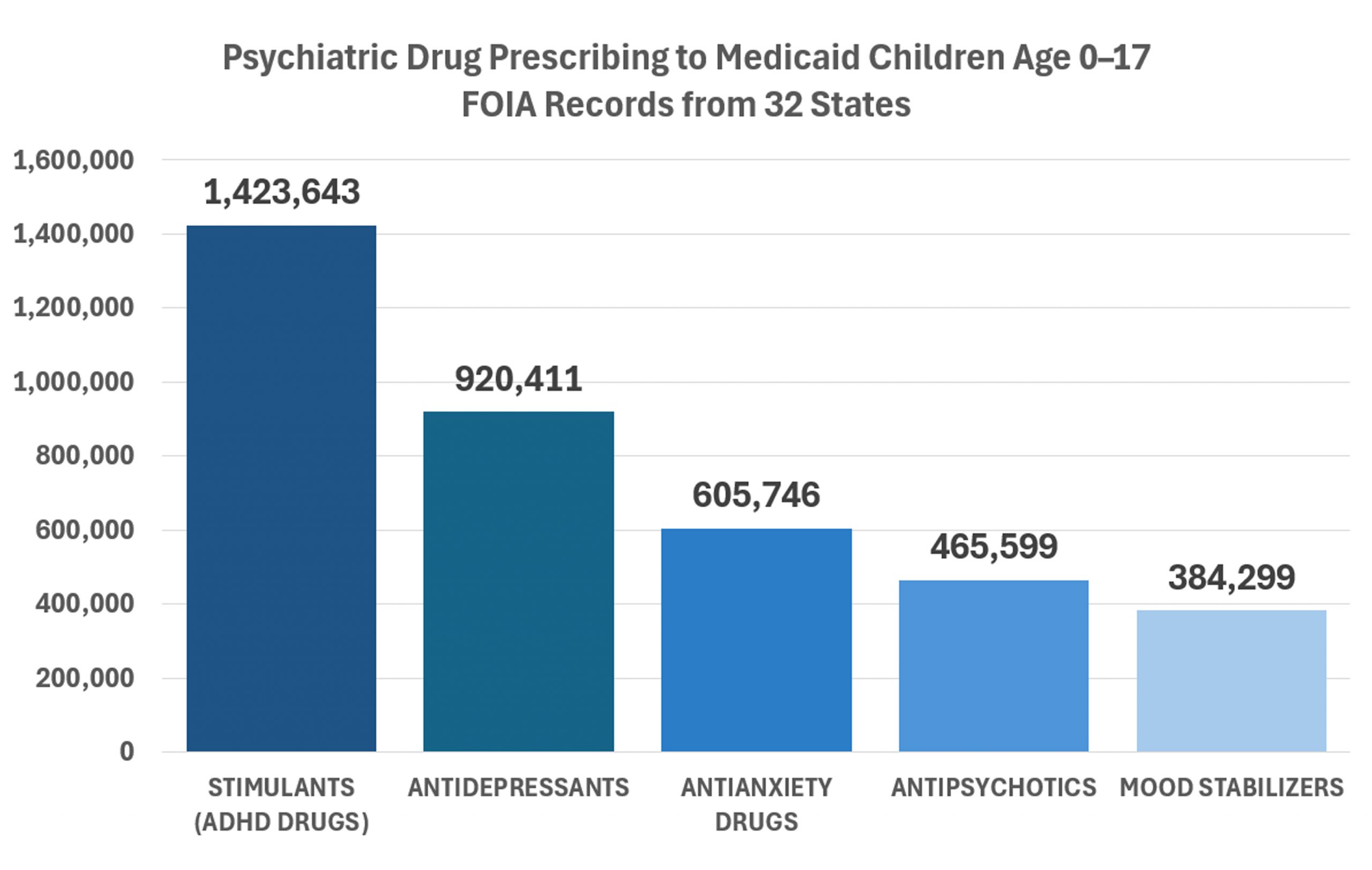
ADHD Drugs: The FOIA data show that ADHD stimulants are the most commonly prescribed psychiatric drugs to children under Medicaid, given to 1,423,643 children aged 0–17, including 89,392 aged 0–5. These are drugs classified by the U.S. Drug Enforcement Administration as Schedule II controlled substances—a category reserved for drugs with a high potential for abuse and addiction, in the same category as OxyContin and fentanyl.
Antidepressants: The second most commonly prescribed class is antidepressants, prescribed to 920,411 children aged 0–17, including 25,414 aged 0–5. These drugs carry a black box warning from the U.S. Food and Drug Administration for increased risk of suicidal thoughts and behaviors in children and adolescents, and clinical research has also documented adverse effects, including agitation, hostility, impulsivity, and emotional blunting or detachment.
Anti-anxiety Drugs: This category including benzodiazepines—are the third most prescribed class, given to 605,746 children aged 0–17, including 145,783 aged 0–5. The FDA warns these drugs carry serious risks of dependence and potentially life-threatening withdrawal reactions.
Antipsychotic Drugs: Prescribed to 465,559 children aged 0–17, including 34,758 aged 0–5. These drugs are associated with severe adverse effects documented in drug safety labeling and research, including diabetes, involuntary movement disorders, cardiovascular risks, and sudden death.
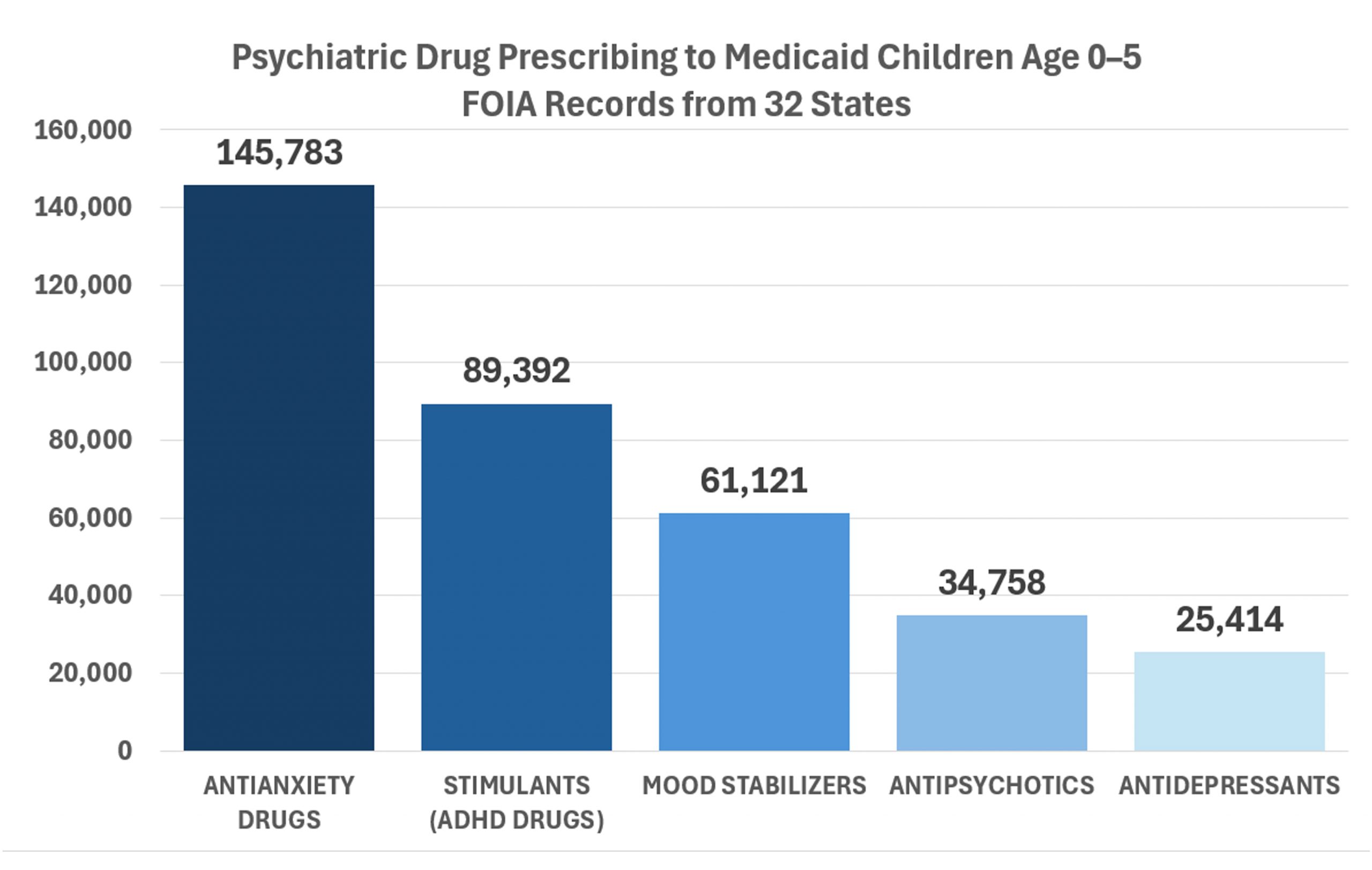
0-5 YEAR OLDS: Most alarming is the drugging of very young children. FOIA data show that 270,196 children aged 0–5 were prescribed psychiatric drugs under Medicaid—including 89,392 on ADHD stimulants, 25,414 on antidepressants, 145,783 on anti-anxiety drugs, and 34,758 on antipsychotics. These are drugs that federal regulators warn carry serious risks—stimulants classified by the U.S. Drug Enforcement Administration as Schedule II controlled substances with high abuse potential, antidepressants carrying a boxed suicide warning from the U.S. Food and Drug Administration, benzodiazepines associated with dependence and life-threatening withdrawal, and antipsychotics linked to diabetes, severe neurological effects, and sudden death.
Evidence of High-Volume Prescribers Operating Within Medicaid With No Scrutiny
CCHR International also filed FOIA requests with states to determine whether the Medicaid system was allowing practitioners to prescribe psychiatric drugs to unusually large numbers of children. The records obtained raise serious concerns that extremely high-volume prescribers are operating within the system with little to no scrutiny. In some cases, individual practitioners billed Medicaid large sums while prescribing powerful psychiatric drugs—including Schedule II stimulant drugs with a high potential for abuse—to hundreds or even thousands of children in a single year.
For example, in the state of Illinois, FOIA records from the Department of Healthcare and Family Services show practitioners prescribing ADHD stimulant drugs to extraordinarily large numbers of Medicaid-enrolled minors with no apparent oversight.
Examples of prescribing volumes include:
- A psychiatric clinical nurse specialist who prescribed ADHD stimulant drugs to 1,674 children in one year—about 32 children per week ($203,711.03 billed to Medicaid).
- A psychiatry physician assistant who prescribed stimulants to 1,033 children—about 20 children per week ($87,690.99 billed).
- A psychiatric nurse practitioner who prescribed stimulants to 988 children—about 19 children per week ($106,154.04 billed).
- A psychiatrist who prescribed stimulants to 985 children—about 19 children per week ($111,023.23 billed).
- A psychiatrist who prescribed stimulants to 962 children—about 18 children per week ($124,064.68 billed).
- A psychiatrist who prescribed stimulants to 898 children—about 17 children per week ($104,249.13 billed).
- A psychiatrist who prescribed stimulants to 827 children—about 16 children per week ($86,179.57 billed).
- A psychiatrist who prescribed stimulants to 801 children—about 15 children per week ($124,860.53 billed).
- A psychiatric nurse practitioner who prescribed stimulants to 749 children—about 14 children per week ($75,980.38 billed).
These figures show that practitioners within Medicaid can prescribe highly addictive stimulant drugs to dozens of children every week while billing the public program significant sums—yet the data indicate these extraordinary prescribing patterns can occur with no scrutiny or oversight.
The following sections provide a detailed analysis of critical policy concerns and necessary reforms if we are to ensure quality safe and effective services are being delivered to this vulnerable population. Each section highlights specific areas where oversight, accountability, and regulatory action are needed to protect patients—particularly children—from the serious risks associated with psychiatric medications.
This report examines:
I. FDA Medication Guides: A Vital Tool for Informed Consent and Safety
II. Mandating Medication Guides as a Condition of Federal Funding for Medicaid
III. Penalties for Medical Care Providers’ Noncompliance with Medication Guide Distribution
IV. Proposal for an Independent FDA-Approved Expert Panel to Review Psychiatric Drug Risks
V. The Need for CMS to Investigate High-Volume Prescribers of Psychiatric Drugs to Children
VI. Establishing a Consumer Adverse Drug Reaction (ADR) Database Under CMS
VII. Penalties for Medicaid Agency Noncompliance with ADR Reporting
Each section outlines actionable recommendations to strengthen informed consent, enhance regulatory enforcement, and ensure taxpayer-funded healthcare programs uphold essential patient protections.
I. THE FDA MEDICATION GUIDES—A VITAL TOOL FOR INFORMED CONSENT
Initiated in 1998 under the U.S. Code of Federal Regulations, the FDA’s Medication Guides (MedGuides) are online fact sheets that provide essential safety information in a non-technical, easy-to-read format listing their most serious side effects. Their development stemmed from concerns that consumers were not receiving adequate and understandable information about potential drug risks.
The FDA mandates that Medication Guides must:
- Use a font size of “no smaller than 10 point.”
- Be written in “nontechnical, understandable” language.
- Avoid promotional tone or content.
- Clearly describe the serious public health concerns necessitating the MedGuide.
- Highlight any known pediatric risks and the potential for dependence on the drug.
Why Parents, Guardians, and Caregivers Need This Information
Without access to FDA-approved Medication Guides, parents and caregivers may not recognize that behavioral changes in their child—such as increased aggression, suicidal thoughts, hallucinations, or severe restlessness—are medication-induced side effects rather than worsening mental health symptoms. This is a direct violation of informed consent. As a result, these reactions may be misinterpreted, leading to unnecessary medication adjustments, additional drug prescriptions, or even psychiatric hospitalizations that could have been prevented with proper awareness of the drug’s risks.
Providing printed copies of FDA Medication Guides to parents, guardians, and state-appointed caregivers ensures they have the information necessary to monitor a child’s response to the drug from the first prescription onward. This is a fundamental safeguard in preventing harm, supporting informed decision-making, and improving oversight in psychiatric drug treatment.
II. MANDATING MEDICATION GUIDES AS A CONDITION OF FEDERAL FUNDING OF MEDICAID
Given that federal Medicaid funds are used to prescribe drugs with serious FDA-documented side effects, it is imperative that the distribution of FDA-approved Medication Guides be required as a condition of utilizing these taxpayer dollars.
Providers should be mandated to:
- Print and distribute FDA Medication Guides at the initial and subsequent prescriptions of psychotropic drugs. (Note: Just the Medication Guide pages, not the entire drug label.)
- Obtain signed consent acknowledging from parents, guardians, or state-designated caregivers that they have been given a paper copy of the Medication Guide and understand the potential risks.
- Require that a physical copy be handed to the parent, guardian, or state-appointed caregiver—not just offered or referenced electronically—and that a signed note, acknowledging they gave the paper copy to them be kept in the patient’s file for future compliance auditing purposes.
Taxpayer dollars should not be spent on psychiatric drugs prescribed to children and adolescents without ensuring that those responsible for a child’s care are fully informed of the potential side effects. Failing to provide this information is a violation of informed consent, denying parents, guardians, and caregivers the ability to make fully informed decisions about a child’s treatment. Enforcing this requirement would strengthen oversight, promote patient safety, and prevent unnecessary medical interventions caused by unrecognized drug side effects.
III. PENALTIES FOR MEDICAL CARE PROVIDERS’ NONCOMPLIANCE WITH MEDICATION GUIDE DISTRIBUTION
I. Denial of Medicaid Reimbursement for Non-Compliant Prescriptions
Any prescription for a psychiatric drug for a minor aged 0–17 issued without documented proof of FDA Medication Guide distribution and signed informed consent shall be ineligible for Medicaid reimbursement. The provider shall bear the full cost of the medication.
- Proof of compliance must include a printed copy of the FDA Medication Guide, signed and dated by the parent, legal guardian, or state-designated caregiver, and retained in the patient’s medical record.
II. Medicaid Charge-Back for Non-Compliant Claims
If a Medicaid audit finds that a provider has failed to comply with the informed consent Medication Guide distribution requirements, Medicaid shall have the right to audit and recoup the payment for the related non-compliant service provided by the Medicaid provider. This may include imposing a chargeback and or require a provider to refund Medicaid for the service fee paid.
III. Permanent Revocation for Repeated or Willful Violations
A provider who violates these requirements three or more times within a 12-month period, after having been given notice by Medicaid of the provider’s failure to be in compliance, or who willfully bypasses informed consent and Medication Guide requirements, shall be permanently prohibited from prescribing psychiatric medications under Medicaid.
IV. PROPOSAL FOR AN INDEPENDENT FDA-APPROVED EXPERT PANEL TO REVIEW PSYCHIATRIC DRUG RISKS
Given the severe, FDA-documented risks of psychiatric drugs prescribed to children—including suicidal ideation, aggression, hallucinations, cardiovascular harm, and developmental delays—it is imperative that an independent, conflict-free review of the existing data be conducted. The FDA already possesses extensive clinical trial data, post-marketing reports, and adverse event findings, yet this information has not been systematically analyzed by experts free from pharmaceutical influence to determine the true scope of harm to children.
The Fair Access to Clinical Trials (FACT) Act, introduced by Senators Chuck Grassley and Christopher Dodd in 2007, played a critical role in increasing transparency in clinical trials. While the bill itself did not pass as a standalone measure, its key provisions were incorporated into the FDA Amendments Act of 2007 (FDAAA), which expanded ClinicalTrials.gov by mandating the registration and public reporting of clinical trial results. This was a significant step forward in ensuring that clinical data is accessible to researchers, policymakers, and the public. However, the law stopped short of requiring independent, systematic reviews of existing clinical trials to evaluate drug safety and efficacy free from industry influence.
Regulatory Failures and Suppressed Evidence: Why Existing Drug Approvals Require Independent Review
The failure to analyze long-held clinical trial data has led to regulatory inaction with life-threatening consequences. One stark example is Dr. Andrew Mosholder’s 2003 review of antidepressant clinical trial data in children, which included trials conducted five to eight years earlier. Mosholder, an FDA epidemiologist, was tasked by the agency to assess the suicidality risks of antidepressants in response to findings from the UK’s Medicines and Healthcare products Regulatory Agency (MHRA), which had determined that SSRIs increased suicidal ideation in children and teens. His review confirmed the UK’s concerns, showing an increased risk of suicidal ideation and behavior in children and adolescents taking SSRIs, with little to no efficacy over placebo. Despite commissioning the analysis, the FDA had never proactively reviewed this data on its own. Rather than acting on Mosholder’s findings, the FDA actively suppressed his report, preventing him from presenting his conclusions at a 2004 advisory meeting. It was only after Congressional scrutiny that the FDA was forced to re-examine the same data and, under public pressure, confirmed Mosholder’s conclusions, ultimately issuing black-box warnings for pediatric antidepressant use on October 15, 2004. This case underscores the urgent need for independent review panels that are free from industry ties and empowered to analyze existing clinical trial data for safety risks that regulators have overlooked or ignored.
Building on the FACT Act: A Conflict-Free Expert Panel to Review Psychiatric Drug Risks
To strengthen oversight beyond transparency, we propose the establishment of an independent, conflict-free expert panel to review the risks of psychiatric drugs. This panel would ensure that regulatory actions are based on comprehensive, unbiased evaluations of existing clinical trial data, rather than being influenced by pharmaceutical industry interests.
The panel’s initial focus shall be pediatric psychiatric drug risks, with the authority to expand its scope to all populations as needed.
I. Structure and Composition of the Panel
The panel shall be composed of FDA-approved, independent experts with no financial ties to pharmaceutical companies, including:
- Clinical Research Associate (CRA) or Clinical Trial Expert
- Biostatistician
- Medical Epidemiologist
- Toxicologist
- Clinical Pharmacologist
- Clinical Safety Reviewer
- Pharmacovigilance Expert
- Regulatory Medical Expert
- Drug Litigation Experts
Conflict-Free Oversight:
- All panel members shall be vetted to ensure no financial conflicts of interest, including no direct or third-party financial ties to pharmaceutical companies.
- The panel shall report directly to the Secretary of Health and Human Services (HHS), the FDA Commissioner, and Congress, not to industry-funded advisory committees.
II. Review Process and Scope
The panel shall conduct a comprehensive, independent review of all existing data on psychiatric drug risks, focusing initially on pediatric populations and expanding as necessary.
1. Ongoing Clinical Trials:
- Review of all currently registered studies involving psychiatric drugs, including those funded by federal agencies and private entities.
2. Completed Clinical Trials:
- Assessment of all trials submitted to ClinicalTrials.gov, including unpublished data that may indicate previously undisclosed risks.
3. Trials Used by the FDA for Drug Approvals:
- Full review of all clinical trials relied upon by the FDA for market approval, including both pre-market and post-market surveillance data.
The Panel Shall Focus On:
- Actual efficacy vs. marketed claims in FDA clinical trial data.
- Documented adverse effects in existing studies and post-market surveillance.
- Rates of polypharmacy (multiple psychiatric drugs prescribed simultaneously) and its impact on patient outcomes.
- Long-term developmental and neurological effects of psychiatric drugs, including FDA MedWatch reports.
- Identification of gaps in current safety monitoring, with recommendations to strengthen consumer protections without requiring new trials that could put patients at additional risk.
II. Transparency and Public Accountability
- All findings shall be published in full and made publicly accessible, unlike past FDA reviews that were influenced by industry interests.
- A Congressional briefing shall be held to ensure policymakers have clear, independent data on psychiatric drug risks.
- The panel shall advise on necessary regulatory actions, including:
- Stronger black-box warnings on high-risk psychiatric drugs.
- Restrictions on off-label prescribing where risks outweigh benefits.
- Increased adverse reaction reporting requirements for Medicaid and federally funded healthcare providers.
IV. Conclusion: Ensuring Oversight Without Industry Influence
The FACT Act helped establish clinical trial transparency, but transparency alone does not ensure regulatory action on known risks. The failure of the FDA to act on critical safety findings—as seen in the case of Dr. Mosholder’s suppressed analysis on antidepressants and suicide risk in children—demonstrates why greater independent oversight is needed.
By establishing an independent expert panel free from pharmaceutical influence, this proposal ensures that scientific evidence, not industry interests, guides psychiatric drug prescribing practices—prioritizing patient safety over profit.
V. THE NEED FOR CMS TO INVESTIGATE HIGH-VOLUME PRESCRIBERS OF PSYCHIATRIC DRUGS TO CHILDREN
The Centers for Medicare & Medicaid Services (CMS) has a direct responsibility to ensure that federal and state Medicaid funds are not being misused to support unsafe prescribing practices—especially for psychiatric drugs prescribed to children. Given the severe, FDA-documented side effects of these drugs, including suicidal ideation, aggression, hallucinations, cardiovascular issues, and developmental harm, there is a pressing need for CMS to actively investigate the top prescribers of these medications to children under Medicaid.
Why CMS Must Investigate High-Volume Prescribers
- Psychiatric Drugs Are Being Prescribed to Children Despite Severe Risks
- FDA warnings on stimulants, antidepressants, and antipsychotics cite life-threatening risks, yet some Medicaid providers continue prescribing them at alarming rates—including to infants and toddlers (ages 0-5) for off-label uses not approved by the FDA, and in some cases not approved for reimbursement under the Federal Medicaid reimbursement guidelines-law.
- CMS must investigate how and why such prescribing occurs, particularly when no long-term safety studies exist for many of these drugs in young children.
- High-Volume Prescribers May Be Engaging in Unsafe or Questionable Practices
- A small percentage of Medicaid prescribers account for a disproportionate number of psychiatric prescriptions for children, often without adequate oversight.
- Some of these prescribers may be:
- Over-relying on psychiatric drugs instead of providing alternative, safer interventions.
- Ignoring FDA black box warnings and pediatric risks.
- Failing to properly monitor children for severe side effects.
- Prescribing multiple psychiatric drugs at once (polypharmacy) significantly increases risks.
- Creating prescribing habits due to pharmaceutical marketing undue influence.
- CMS must track and audit the highest prescribers, identify prescribing patterns that deviate from safety guidelines, and take corrective action when necessary.
- Accountability for the Use of Federal Medicaid Funds
- Since Medicaid is a publicly funded program, CMS has an obligation to ensure taxpayer dollars are not facilitating reckless prescribing or the overmedication of vulnerable children.
- Unlike private-sector patients, Medicaid beneficiaries often lack the ability to refuse treatment, making strong oversight even more critical to prevent harm and misuse of psychiatric medications.
- Federal funding should not support prescribing practices that expose children to serious harm without adequate safeguards in place.
Required CMS Actions
To address these concerns and protect child safety, CMS must:
- Identify and Monitor the Top 10% of High-Volume Medicaid Prescribers of Psychiatric Drugs to Children
- Require state Medicaid agencies to provide quarterly reports on the highest prescribers of stimulants, antidepressants, mood stabilizers, antipsychotics, anti-anxiety drugs and sedatives to children.
- Investigate providers who prescribe psychiatric drugs to children under 5 years old, as nearly all such prescriptions are off-label and lack FDA approval and CMS reimbursement approval for this age group.
- Eliminate the use of supporting compendia to justify ignoring FDA age restrictions or off-label use of psychiatric drugs with severe side effects as noted by the FDA.
- Conduct Targeted Audits and Oversight of High-Risk Prescribers
- Audit prescribers with an unusually high rate of psychiatric prescribing compared to state and national benchmarks.
- Review patient records to determine whether informed consent, appropriate monitoring, and alternative treatment options were considered before prescribing.
- Require corrective actions for providers whose prescribing patterns raise safety concerns.
- Implement Restrictions for High-Risk Prescribers
- Mandate prior authorization for psychiatric drug prescriptions when prescribed by providers flagged for excessive psychiatric drug prescriptions to children and adolescents.
- Prohibit polypharmacy of psychiatric drugs in children under Medicaid.
- Establish a disciplinary framework, including warnings, and removal from the Medicaid program for prescribers engaging in unsafe practices.
Conclusion
The widespread prescribing of high-risk psychiatric drugs to children under Medicaid must be met with serious federal scrutiny. CMS must take an active role in monitoring, investigating, and regulating the top prescribers of these drugs to ensure that public funds are not being used to support reckless prescribing practices that endanger children. By enforcing data-driven oversight and accountability measures, CMS can help prevent unnecessary drug exposure, reduce severe adverse effects, and protect the health and safety of vulnerable children.
VI. ESTABLISHING AN ADVERSE DRUG REACTION (ADR) DATABASE UNDER CMS
Lack of a Medicaid-Funded Adverse Drug Reaction Reporting System
A reliable system for reporting adverse drug reactions (ADRs) to psychiatric medications is critical for monitoring their effects on children. Currently, there is no accessible Medicaid-funded mechanism to report and track ADRs, limiting the ability to identify and address medication-related harms. This lack of oversight leaves children vulnerable to prolonged exposure to dangerous drug effects without proper intervention.
Medicaid’s Responsibility to Ensure Safety and Oversight
Given that Medicaid is the primary payer for psychiatric prescriptions for children in the public sector—including off-label use in very young children—it has a direct responsibility to ensure safety and oversight. Establishing an online ADR reporting system would enable Medicaid agencies and legislators to track the frequency and severity of adverse reactions, support evidence-based decision-making, and enhance public health protections for children receiving psychiatric medications.
I. The Need for a Medicaid-Specific Adverse Drug Reaction Online Reporting System
Currently, there is no federally mandated adverse drug reaction (ADR) reporting system within Medicaid to track the effects of psychiatric drugs prescribed to children under federal and state-funded healthcare programs. Medicaid is the largest public payer for psychiatric drugs in children, including their off-label use in those as young as 0–5 years old. However, adverse reactions to these drugs are not systematically tracked within the Medicaid system, leaving policymakers and agencies without the data necessary to ensure patient safety.
While the FDA’s MedWatch system allows patients, healthcare professionals, and pharmacists to voluntarily report ADRs, it primarily serves private-sector medical settings and does not collect data specifically linked to Medicaid-funded prescriptions. The MedWatch system is also difficult to navigate for nonprofessionals. Given that Medicaid funds are being used to cover these drugs, the Centers for Medicare & Medicaid Services (CMS) must have direct awareness of the adverse effects their funded medications are causing. Without this oversight, Medicaid agencies remain unaware of the frequency, severity, and nature of medication-related harms occurring in the most vulnerable pediatric populations.
A Medicaid-specific ADR reporting system would establish a direct, efficient, and accountable mechanism for tracking adverse effects in children prescribed psychiatric drugs. Unlike MedWatch, which requires complex submission processes and is often underutilized, this system would be designed to be streamlined, user-friendly, and accessible to parents, guardians, and caseworkers—those most directly witnessing adverse effects in children. Like the Medication Guides available by the FDA, the Medicaid-Specific Adverse Drug Reporting (MS.ADR) system would use common and simple language.
II. Streamlined Reporting System for Better Data Collection
The state Medicaid agency shall, within 12 months of this Act’s enactment, develop and maintain a secure online MS.ADR reporting system dedicated to psychiatric drugs prescribed to children and adolescents. This system shall simplify and streamline reporting to encourage participation, ensure faster data processing, and reduce errors. Features will include:
- User-friendly interface with free-text fields and dropdown menus for categorization.
- Required fields for patient information, prescribing doctor information, drug details, and adverse effects to ensure accuracy.
- Pre-set categories for adverse reactions (physical, psychological, behavioral) to facilitate data analysis.
- Optional contact fields for follow-up to enable further investigation when necessary.
By making the system efficient and easy to use, it removes barriers to reporting, ensuring timely and comprehensive data collection that can inform Medicaid policies and protect children.
III. Adverse Drug Reaction Reporting Requirements for Medicaid Agencies
Medicaid agencies shall be required to compile and submit quarterly reports summarizing ADR data related to psychiatric drugs prescribed to children. These reports will be submitted to CMS and shall include:
- The number of ADRs reported by patient age.
- Severity levels of ADRs categorized as mild, moderate, or severe.
- A breakdown of ADRs by reaction type (physical, psychological, behavioral).
- Trends in ADRs linked to specific drug classes.
This requirement will provide CMS with data-driven insights into medication safety, allowing them to assess the impact of psychiatric prescribing practices and take corrective action as needed.
VII. PENALTIES FOR MEDICAID AGENCY NONCOMPLIANCE WITH ADVERSE DRUG REACTION (ADR) REPORTING
The penalties in this section shall apply only if the Medicaid agency has a structured database capable of tracking adverse drug reaction (ADR) reports and compliance records.
I. Monetary Penalty for Failure to Submit ADR Reports
If the Medicaid agency fails to submit the required ADR reports to the appropriate legislative committees within 30 days of the deadline, it shall incur a monetary fine for each quarter of noncompliance, with fines increasing for repeated violations.
- All collected fines shall be directed to a dedicated state fund for improving Medicaid oversight and drug safety measures.
II. Reduction in Medicaid Funding for Ongoing Noncompliance
If the Medicaid agency fails to submit two or more consecutive ADR reports, the state Medicaid program shall have its administrative funding reduced for the following fiscal quarter until full compliance is demonstrated, including the timely submission of all required ADR reports.
III. Oversight Review for Recurring Failures
If the Medicaid agency fails to comply with ADR reporting requirements for three or more quarters in a fiscal year, the Governor or relevant state oversight body shall initiate a formal review of the Medicaid agency’s operations and reporting procedures. This review may result in corrective actions, including the appointment of an external auditor to ensure the accurate and timely reporting of ADR data.
SHARE YOUR STORY/COMMENT