
Psychiatrists’ misleading claims could deny consumers evidence of ECT’s real damage, inducing suicide
By Jan Eastgate
President, CCHR International
The Mental Health Industry Watchdog
July 2, 2019
In a requested statement provided to The Wall Street Journal regarding the use of electroshock treatment (ECT), the mental health watchdog group, Citizens Commission on Human Rights, stated: “With no clinical trials proving its safety, electroshock treatment plays Russian roulette with the lives of vulnerable people who are often ill-informed about its long-term effects, including, according to an ECT device manufacturer, permanent brain damage, as well as severe memory loss.” It can also “cause, not prevent suicide. Law suits and coroners inquests confirm this, reinforcing the need to ban the torturous practice and insist upon workable, non-invasive treatments that do not harm.”
This was not reported, yet had the inquests, lawsuits and studies upon which the statement was made been researched, the information that electroshock-doctors provided to the WJS would have been refuted, giving consumers and their families some necessary warnings.
The article included the usual disclaimers that ECT “still causes memory loss,” people may have “difficulty forming memories for a few weeks or months after the treatment,” but that newer technology reduces this. However, experts say this is inaccurate, ignoring serious adverse events, including brain damage, which can be permanent.
Rather than prevent suicide—as psychiatrists claimed in the WSJ article—ECT can induce suicide. That would have been important information for readers to know.
- A UK coroner investigating the death of a mother of one in 2016 found that the ECT she’d been administered had led to a “deterioration in her mental health…culminating in her decision to commit suicide.”[1]
- A coroner’s inquest in Australia in 2017 determined that involuntary ECT did not prevent but may have led to a patient’s death after a suicide attempt.[2]
- Also in 2017, UK researchers reviewed more than 90 ECT studies since 2010 and determined: “There is still no evidence that ECT is more effective than placebo for depression reduction or suicide prevention.”[3]
Other unqualified psychiatric statements included that ECT is somehow less risky today because shorter pulses of electricity reduces the brain’s exposure to it and electrodes are placed on one side of the head instead of both. Taking their information at face value, the WSJ reported that advances in technology and technique have reduced the severity of memory loss, albeit not eliminating this risk. It also theorized that ECT helps to “realign disrupted circuits,” without citing any evidence to support this.
Other theories are that the grand mal seizure that ECT causes is a therapeutic. However, as Kenneth Castleman, Ph.D. says, the scientific literature fails to establish a mechanism of therapy or to support the belief that the seizures produced by ECT are therapeutic. Further, the amount of electricity that is used in practice is routinely at least six times what is required to produce a seizure.[4]
Of such theories, he says: “The opinion of ‘authorities in the field’ is being substituted for scientific fact.” Castleman has a Bachelor and Master’s degrees in electrical engineering and a Ph.D. in Biomedical Engineering. The latter involves application of engineering techniques to problems in medicine and biology. His entire professional career has been dedicated to scientific research and technology development. He has served on various university and government advisory committees and was a Senior Scientist at NASA for 15 years. He says any newer ECT procedure does not reduce the damage, with data as follows.
- In ECT, the voltage is as high as 460 volts and creates an electric field inside the patient’s skull. This electric field puts a force on the electrons inside the brain, causing them to move. This movement of electrons is a current flow of up to 900 mill amperes. By contrast, brain cells normally operate with less than one-half of a volt and a fraction of one milliamp ere.[5]
- Two things happen when an electric current flows through the brain: Electrical energy is converted into heat inside the brain, raising its temperature. The larger the current, the more heat is produced. If the temperature gets too high the cells will suffer temporary injury, permanent damage, or even death.
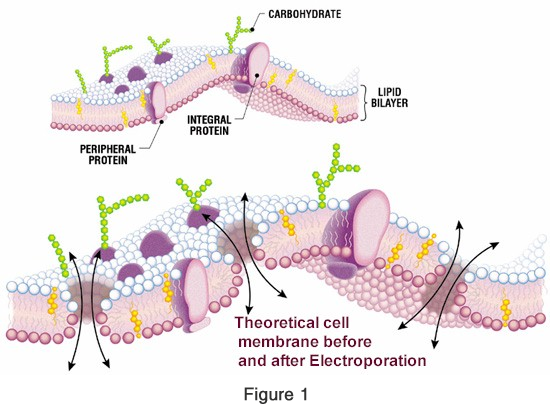
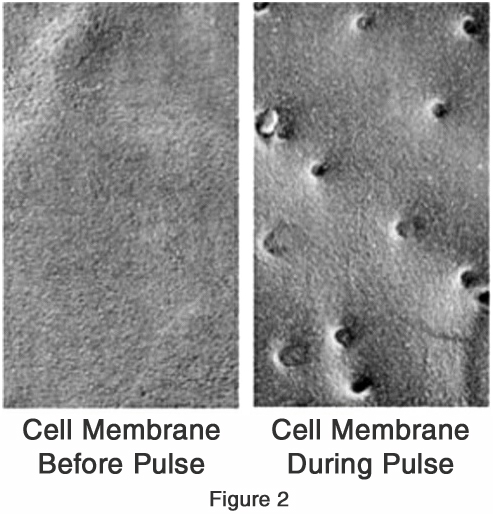
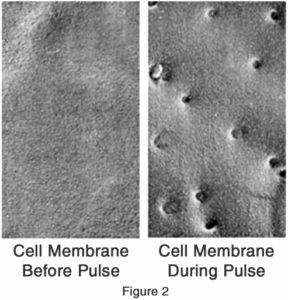 The second effect results from the pulsing nature of the voltage applied by ECT machines. This process of alternately pulling and tugging on the cell membrane creates a jackhammer effect that can tear holes in cell walls. This process is called “electroporation,” the creation of pores (holes) in the cell wall by electrical means.[6] As little as one volt across the cell membrane can open holes. Today’s Modern Brief-Pulse and Ultrabrief Pulse ECT devices are much more likely to cause electroporation than those used in the past.
The second effect results from the pulsing nature of the voltage applied by ECT machines. This process of alternately pulling and tugging on the cell membrane creates a jackhammer effect that can tear holes in cell walls. This process is called “electroporation,” the creation of pores (holes) in the cell wall by electrical means.[6] As little as one volt across the cell membrane can open holes. Today’s Modern Brief-Pulse and Ultrabrief Pulse ECT devices are much more likely to cause electroporation than those used in the past.
- The amount of electric current that an ECT machine puts through a patient’s head is approximately 100 times what Tasers, cattle prods, and electric fences use, about the same as what is used for stunning pigs, and roughly one-fifth as much as the electric chair. In addition, the amount of voltage applied to the head (460 volts) is about 400 times what is required to damage a single brain cell. Clearly this amount of electricity has the potential to cause injury to the brain.
And yet despite all this potential damage, psychiatrists boast in the article how studies have been conducted to treat the symptoms of dementia, such as aggression and agitation in the elderly with dementia. Those aged 50 and older and referred for ECT were used in one study.
There was no questioning in the WSJ article about the ethics and rationale behind the Food and Drug Administration’s (FDA) decision last December to lower the risk classification of the ECT device to moderate-risk Class II risk for three disorders that does not include dementia. And whether conflicts of interest may have influenced the decision, when it was clear the ECT device makers had refused to conduct the necessary Class III device clinical trials Congress requires to prove safety and efficacy in order to remain on the market under the Federal Food, Drug, and Cosmetic Act.
Rather, ECT is projected as an option for so-called “treatment-resistant depression,” an arbitrary—not medically or scientifically-based—term to obscure treatment failures.
Dr. Allen Francis, former head of the APA’s fourth edition of its diagnostic manual, also says, “We use terms like treatment-resistance and treatment-refractory, but this is merely an admission of our failure to have a solution.” Further: “We persist in treatment, usually by giving whatever has failed previously in more dosage or by adding new treatments that have little chance of success, but a high risk of side effects.”[7]
CCHR says the FDA, APA and all shock-delivering psychiatrists should study electricity to understand fully what it does to damage the brain, causing cell death and learn from Australian psychiatrist, Niall McLaren who wrote that any psychiatrist who says, “‘You need ECT’ is really only saying, ‘I don’t know what else to do.’ I will repeat: No psychiatrist needs to use ECT.”[8]
References:
[1] “Mental health service failure “significantly contributed” to suicide of Norwich mother,” Eastern Daily Press, 18 Apr. 2018, https://metro.co.uk/2018/04/20/why-is-electric-shock-treatment-still-given-in-2018-7475746/?ito=cbshare
[2] https://www.theage.com.au/national/victoria/grandfather-forced-to-undergo-ect-before-preventable-death-20180418-p4zacy.html
[3] John Read and Chelsea Arnold, “Is Electroconvulsive Therapy for Depression More Effective Than Placebo? A Systematic Review of Studies Since 2009,” Ethical Human Psychology and Psychiatry, Vol. 19, No. 1, 2017, http://www.ingentaconnect.com/content/springer/ehpp/2017/00000019/00000001/art00002
[4] Kenneth R. Castleman, Ph.D., Castleman citing, MECTA Corporation, MECTA Instruction Manual, SPECTRUM 5000Q, SPECTRUM 4000Q, SPECTRUM 5000M, SPECTRUM 4000M, Revision 06, November 7, 2008; R Abrams & CM Swartz, “THYMATRON® System IV Instruction Manual – Twelfth Edition,” UM-TS4, Rev. 12, Somatics LLC, May, 2006.
[5] Kenneth R. Castleman, Ph.D., “How Electroshock ‘Works,’” https://www.cchrint.org/ect-basics/
[6] Castleman citing, RC Lee, “Cell Injury by Electric Forces,” (Review Article) Ann. N Y Academy of Sciences, 1066: 85-91, Dec. 2005; RC Lee, et al., eds., Cell injury: mechanisms, responses, and repair, New York Academy of Sciences, 2005. ISBN 978-1-57331-616-3; JC Weaver, “Electroporation of Cells and Tissues,” IEEE Transactions on Plasma Science, 28(1):24-33, Feb. 2000; WA. Hercules, et al., Electroporation of Biological Cells Embedded in a Polycarbonate Filter, Howard University, Washington, D.C. 2003. https://arxiv.org/ftp/physics/papers/0308/0308015.pdf; M Kanduser and D Miklavcic, “Electroporation in Biological Cell and Tissue: An Overview,” in E Vorobiev, N Lebovka (eds.), Electrotechnologies for Extraction from Food Plants and Biomaterials, DOI: 10.1007/978-0-387-79374-0 1, Springer Science and Business Media, LLC, 2008; JH. Rossmeisl Jr. “Pathology of non-thermal irreversible electroporation (N-TIRE) -induced ablation of the canine brain,” J. Vet. Sci., 14(4), 433-440, 2013. http://dx.doi.org/10.4142/jvs.2013.14.4.433
[7] Allen J. Frances, M.D., “What to Do When Treatment Doesn’t Work,” Psychology Today, 29 Jul. 2016, https://www.psychologytoday.com/us/blog/saving-normal/201607/what-do-when-treatment-doesnt-work
[8] Niall McLaren, “No Psychiatrist Needs to Use ECT,” 27 June 2017
SHARE YOUR STORY/COMMENT